Nervous System Pathology Slides
|
||
|
K NS-52 & K NS-53 |
|
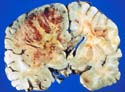
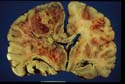
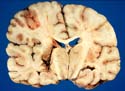
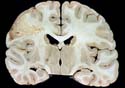
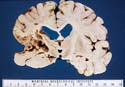
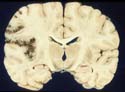
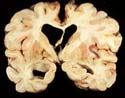
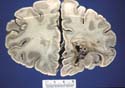
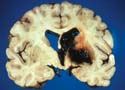
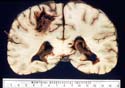
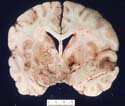
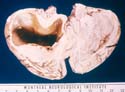
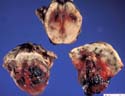
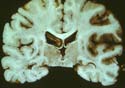
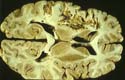
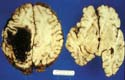
These are pictures of coronal sections of the cerebrum of a patient with glioblastoma. Note the expansion and destruction of the left cerebral hemisphere by the tumor, the narrowing of the body of the left lateral ventricle and herniation of the lower part of medial face of the hemisphere under the free margin of the falx cerebri. In the tumour, viable tumour tissue is pale grey-pink; the yellow tissue is necrotic and there are numerous hemorrhages in the zone between necrotic and viable tumour. |
|
K NS-54 |
|
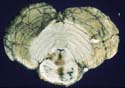
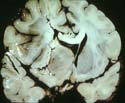
Horizontal section through the upper brain stem of the patient shown in the two previous slides. This shows that death is due to secondary brain stem pressure hemorrhages. |
| K NS-120 | 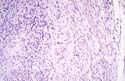 |
Photomicrograph of Schwannoma. Same case as K NS-117 and 118. Project picture so that free tissue surface is on your right. The left half of the field is occupied by the Schwannoma, the right by part of the S1 dorsal root from which the tumour has arisen. Identify axons and myelin sheaths in this root. |
|
K NS-56 |
|
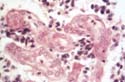
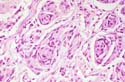
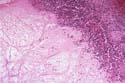
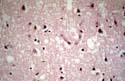
Detail of blood vessels within a glioblastoma multiforme. There is exuberant proliferation of plump endothelial cells. This is a characteristic feature of glioblastoma. |
| K NS-55 | 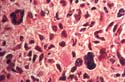 |
Photomicrograph of glioblastoma multiforme showing cells with large hyperchromatic nuclei set in a fibrillary background. |
|
K NS-58 |
|
Photomicrograph showing typical features of meningioma. |
| K NS-57 | 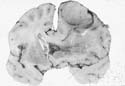 |
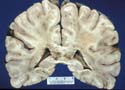
Coronal section of the cerebrum of an elderly patient with a large convexity meningioma. Note the relationship of the tumour to the brain and the pressure features. |
| K NS-59 | 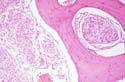 |
Meningioma permeating trabecular spaces of bone of the skull. |
|
K NS-118 |
|
Operative view of spinal Schwannoma before its excision. The dura has been opened longitudinally and retracted by four black linen sutures. The glistening arachnoid membrane can just be detected by the reflections of the lights. The elongated structures are nerve roots. The smooth, bulging tumour is displacing them medially. The epidural space is packed off with lintine strips. Same case as K NS-117. |
| K NS-117 |  |
Myelogram. Orient yourself by identifying bony structures. Study the opacification of the lumbo-sacral subarachnoid space which has resulted from introduction of contrast medium. Note the smoothly contoured defect in the contrast column produced by an intradural mass. |
| K NS-119 | 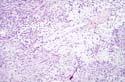 |
Photomicrograph of Schwannoma. Same case as K NS-117. Note the two tissue patterns present: closely packed elongated cells in bundles (Antoni type A) and loosely arranged cells with stellate outlines (Antoni type B). |
|
K NS-3 |
|
This coronal slice of the cerebrum is viewed from its posterior aspect. You will (about 3 days duration) recognize a large recent cerebral infarct involving left middle cerebral artery territory. Note swelling of the left hemisphere, smallness of the body of the left lateral ventricle. |
|
K NS-5 |
|
This is a coronal slab of cerebrum. A cerebral infarct of partial left middle cerebral artery distribution is well demarcated, and the necrotic tissue is beginning to break down. This lesion is of about 2 weeks' duration. Note that cerebral swelling is no longer present and, if anything, the ipsilateral ventricle is larger than the contralateral. |
|
K NS-6 |
|
This is a coronal section of cerebrum from a patient who had a right hemiparesis of several years' duration. It shows an old cavitated infarct within the territory of the left middle cerebral artery. Note that there are also small isolated infarcts in anterior cerebral territory bilaterally. This patient had severe stenosis of his left internal carotid artery. |
|
K NS-11 |
|
Some seven weeks before death this patient became dizzy, drowsy, and lethargic. Her speech was said to be jumbled. Within two hours, she had lapsed into coma. During her seven weeks in hospital, she remained comatose and had to be tube fed. The picture shows an infarct involving both sides of the pons. It resulted from thrombosis of the basilar artery. |
|
K NS-12 |
|
A view of the aortic valve with endocarditis and large nodular vegetations on the aortic cusps. |
|
K NS-14 |
|
This coronal section of brain shows a recent embolic infarct in middle cerebral territory. Note the hemorrhagic nature of the lesion in the cortex and its pallor in the white matter. Note also the swelling of the involved hemisphere. |
|
K NS-15 |
|
The photograph shows a coronal section of the brain of a young man who jumped suicidally from a high window and fractured both femurs. He died on the third hospital day of massive fat embolism. Note the numerous perivascular hemorrhages, especially into the corpus callosum. |
|
K NS-16 |
|
This is a close-up of corpus callosum from case K NS-15 |
|
K NS-17 |
|
This frozen section, stained with Sudan IV, showed a branching capillary crammed with fat lobules from the case illustrated in the previous two slides. |
|
K NS-18 |
|
This close-up photograph shows a saccular aneurysm arising in the angle of bifurcation formed by the division of the internal carotid artery into anterior and middle cerebrals. |
|
K NS-19 |
|
A view of the base of the brain with the arachnoid dissected away to show the major constituents of the Circle of Willis. An unruptured aneurysm arises from the anterior communicating artery and its fundus projects downwards. |
|
K NS-20 |
|
A photomicrograph of a section of cerebral artery (on the left) showing the point of origin of a saccular aneurysm (on the right). Note that the internal elastic lamina (stained black) and the muscularis stop abruptly at the point of origin of the aneurysm, the wall of which is formed by quite delicate connective tissue. |
|
K NS-21 |
|
A view of the base of the brain of a patient who died of a massive subarachnoid hemorrhage from rupture of a saccular aneurysm. Note the extensive subarachnoid haemorrhage at the base of the brain obscuring the aneurysm. |
|
K NS-22 |
|
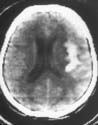
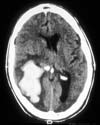
A horizontally oriented CT scan of the head of a patient with subarachnoid hemorrhage forming a subarachnoid hematoma in the right insular region. Compare with next slide, K NS-23. |
|
K NS-23 |
|
A coronal section of the brain of a patient with an abundant subarachnoid hematoma occupying the insula in a patient who had a ruptured aneurysm on the right middle cerebral artery. |
|
K NS-24 |
|
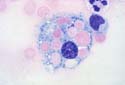
A high power view of cells in the CSF of a patient on the second day of a subarachnoid hemorrhage. Note the large phagocytic cell in the centre with numerous ingested red cells. |
|
K NS-25 |
|
A close-up view of the base of a brain of a patient with two saccular aneurysms, the fundi of which are embedded in the brain substance. Identify the cut end of the internal carotid artery, which is held by artery forceps, the optic nerves, mamillary bodies, and bifurcation of the basilar artery. One aneurysm arising from the bifurcation of the internal carotid where it forms the anterior and middle cerebral arteries is partially buried in the under-surface of the left frontal lobe. A second aneurysm arising from the left middle cerebral artery has its fundus embedded in the temporal lobe. |
|
K NS-26 |
|
This is from the same case as slide K NS-25. Here the aneurysms have been dissected out of the brain and placed upon white cardboard for photographic contrast. A window has been cut in the undersurface of the left temporal lobe to expose a large intracerebral hematoma. |
|
Which additional physical signs might be produced by the presence of an intracerebral hematoma in case of a ruptured saccular aneurysm? |
||
|
How would the presence of such a hematoma affect clinical management of the patient? |
||
|
K NS-28 |
|
A coronal section of the cerebrum from a patient who had a ruptured anterior communicating aneurysm several weeks before death. He remained stuperose throughout his hospital stay. Note the bilateral anterior cerebral infarcts and the two small cavitated infarcts in the left globus pallidus. |
|
The ventricular system is moderately dilated. What factors might contribute to this? |
||
|
K NS-29 |
|
A coronal section of the frontal lobes of the brain of a patient who died of unrelated causes. Note the presence in the right hemisphere of an arterio-venous malformation with surrounding cavitation and staining of the brain tissue. |
|
K NS-30 |
|
A photomicrograph of a small perforating artery (lenticulo-striate artery) in the brain of a patient with severe arterial hypertension who died of massive intracerebral hemorrhage. Note the eccentric hyaline thickening of the vessel wall and presence of occasional foamy macrophages. This change is sometimes referred to as lipohyalinosis. |
|
K NS-31 |
|
A coronal section of the brain of a patient with severe arterial hypertension who died 36 hours after a right capsular hemorrhage. Note the medial rupture of the hematoma to fill the right lateral and third ventricles with blood clot. |
|
What major clinical signs would you expect this patient to have shown? |
||
|
K NS-32 |
|
A horizontal section of the brain of a patient who died shortly after developing a massive left intracerebral hemorrhage. Note the extensive destruction of deep structures within the hemisphere and displacement of midline structures to the right. |
|
K NS-33 |
|
Two horizontal sections of the brain stem and adjacent cerebellum of a patient with a massive hypertensive pontine hemorrhage. |
|
K NS-34 |
|
Horizontal section of the pons and cerebellar hemispheres from a patient with hypertensive cerebellar hemorrhage. Note that rupture into the fourth ventricle has not yet taken place. Also, there is some satellite hemorrhage on the left (contralateral) side. |
|
K NS-35 |
|
An intraoperative view of the surface of the brain of a young man with an arterio-venous malformation. You are looking at the central region of the left cerebral hemisphere. The vertex of the brain is towards the lower part of the picture and the patient's nose off to the right side. Abnormally large red veins are seen towards the bottom of the picture where the blood is drained from the shunting malformation into the superior sagittal sinus. |
|
K NS-36 |
|
The brain at autopsy from the patient shown in slide K NS-35. Note how much less dramatic the surface lesion appears now that circulation has stopped. The dark lesion within the left hemisphere is partly intracerebral hematoma, but much of it is made up by abnormal vascular channels. |
|
K NS-37 |
|
This is a close-up view of the intracerebral lesion from slide K NS-36. In the lower part of the lesion, widely open abnormal blood vessels are seen. |
|
K NS-38 |
|
A picture of a myelin stained section of the medulla showing a wedge-shaped lesion (pale) in the lateral portion of the medulla. It is on the right side. This is from Case 2, Session 1. |
|
K NS-40 |
|
Convexity of the brain of an adult with Hemophilus influenzae meningitis. Note the prominent engorged veins and the subarachnoid purulent exudate most easily seen alongside the veins. |
|
K NS-41 |
|
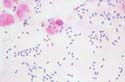
Gram stained film of centrifuged CSF of a patient with S. pneumoniae meningitis. |
|
K NS-44 |
|
Base of the brain in a patient with tuberculous meningitis. Notice the abundant tenacious fibrinous exudate filling the basal cisterns. |
|
K NS-45 |
|
Coronal section of the brain of a patient with tuberculous meningitis. Note the extensive infarction of basal structures as a consequence of obliterative arteritis. These lesions determine the irreversibility of tuberculous meningitis in the late stages of its evolution. |
|
K NS-46 |
|
Subarachnoid exudate of tuberculous meningitis. Note the abundant fibrin and cellular exudate undergoing necrosis. |
|
K NS-47 |
|
Obliterative arteritis in tuberculous meningitis. |
|
K NS-48 |
|
Multiple right temporal lobe abscesses. The whole of the right cerebral hemisphere is swollen because of edema. Note the displacement of mid-line structures to the left. Two of the abscesses have well defined walls and between them there is a dark area of spreading cerebritis. |
|
What are the likely cause or causes of death in this patient? |
||
|
K NS-49 |
|
Photomicrograph of the margin of an abscess at an early stage of its evolution. The upper part of the picture is occupied by pus and the lower part by brain tissue. Notice the well defined junction and lack of granulation tissue at this early stage. |
|
K NS-50 |
|
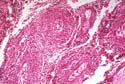
The capsule of an abscess is formed by proliferation of connective tissue from the adventitia of blood vessels. In this photomicrograph note the expansion of the connective tissue of the blood vessels and the chronic inflammatory infiltrate in this region. |
|
K NS-60 |
|
Astrocytoma in the thalamus of a 12-year-old child. Note the loss of the usual anatomical markings of the affected thalamus. |
|
K NS-61 |
|
Cystic cerebellar astrocytoma. Cerebellar astrocytomas usually occur in children, are frequently cystic and in many cases can be completely excised to give a complete cure. |
|
K NS-62 |
|
Photomicrograph of an astrocytoma showing microcystic change. The nuclei are uniform in size and shape. Blood vessels are inconspicuous. Compare this with the microscopic appearance of glioblastoma (slides K NS-55 & 56). |
|
K NS-68 |
|
Schwannoma is present in the right cerebello-pontine angle. It arises from the eighth cranial nerve. This is a case from 1956, and you should not be given the opportunity to see another example at autopsy, as this lesion is eminently amenable to surgical removal. |
|
K NS-69 |
|
Metastatic malignant melanoma. There are two melanoma deposits in the right hemisphere and two in the left. Note the extensive hemorrhage with one deposit. |
|
K NS-70 |
|
Metastatic carcinoma in the brain. Note the extensive edema of white matter and consequent subfalcal herniation. It is characteristic of metastatic carcinoma deposits that they induce great edema of the surrounding white but not grey matter. |
|
K NS-72 |
|
Upper control mid-brain. Lower. Patient with Parkinson's disease. Note depigmentation of substantia nigra and grey-brown discoloration secondary to gliosis. |
|
K NS-73 |
|
Parkinson's disease. Lewy bodies. Hematoxylin and eosin stain. |
|
K NS-74 |
|
Motor neuron disease (amyotrophic lateral sclerosis). Note changes in descending, (motor) tracts. |
|
K NS-75 |
|
Motor neuron disease (amyotrophic lateral sclerosis). Hematoxylin and eosin-Luxol fast blue stain. Anterior horn of thoracic cord. Note absence of motor neurons with proliferation of astrocytes. |
|
K NS76 and 76A |
|
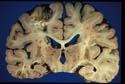
Each slide shows two coronal slabs of brain. That on the right in each slide is a normal control. That on the left is from a patient with Alzheimer’s disease. Note small overall size, widened sulci (especially insulae), dilated ventricles and small hippocampi. |
|
K NS77 |
|
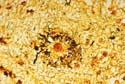
High power view of a senile (neuritic) plaque from a patient with Alzheimer’s disease. The small central disc is a deposit of amyloid. It is surrounded by a ring of dark staining processes; these are dystrophic neurites (process of nerve cells). The section was stained by Bielschowsky’s method which stains axons. |
|
K NS78 |
|
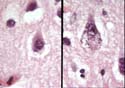
A single neurone is seen in each of the two panels. The one on the right contains a tangle: that on the left is normal. Bielschowsky’s silver method for tangles. |
|
K NS79 |
|
In this two panel slide the left panel shows normal neurones. The right panel shows a neurone with granulo-vacuolar change; note vacuolated appearance of cytoplasm and fine dark staining dots. From a patient with Alzheimer’s disease, HE stain. |
|
K NS-81 |
|
Pick's disease. Note cortical atrophy, particularly prominent in frontal and temporal lobes, but sparing the posterior portion of the superior temporal gyrus. |
|
K NS-84 |
|
Watershed infarcts. Note infarcts in the watershed between the anterior cerebral and middle cerebral arteries, and in the watershed between the middle cerebral and posterior cerebral arteries. |
|
K NS-85 |
|
Watershed infarcts. This coronal section of the cerebral hemispheres is taken more caudal than K NS-84, which is from the same case. Note that there is infarction of the cortex as well as white matter in the watershed between the anterior and middle cerebral arteries and in the watershed between the middle and posterior cerebral arteries. |
|
K NS-86 |
|
Necrosis of Sommer's sector of hippocampus. |
|
K NS-87 |
|
Wernicke-Korsakoff syndrome. Medulla oblongata. Note brownish discoloration of the floor of the fourth ventricle involving particularly vestibular nuclei. |
|
K NS-91 |
|
Cerebellum and one level of medulla. Atrophy of superior part of vermis of cerebellum in a chronic alcoholic. |
|
K NS-98 |
|
Multiple sclerosis. Coronal section of cerebral hemispheres. Note MS plaques at the angles of the lateral ventricles and adjacent to one temporal horn. MS plaques also seen within the internal capsule. |
|
K NS-99 |
|
Multiple sclerosis. MS plaque, close-up. |
|
K NS-100 |
|
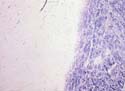
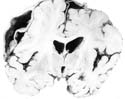
Multiple sclerosis. Heidenhain stain. This stain renders myelin black. Note sharp demarcation of normal myelin and demyelination of MS plaque. |
|
K NS-102 |
|
Multiple sclerosis. Upper pons and cerebellum. Upper half: Heidenhain stain from myelin. Lower half. Holzer stain for astrocytes. Note the well demarcated area of myelin loss, accompanied by gliosis, such that the stain for myelin is a mirror image of the stain for astrocytes. |
|
K NS-104 |
|
Autopsy appearance of an extradural (epidural) hematoma in a 19 year old man. You are looking at the top of the head after removal of the vault of the skull but before cutting the dura. Note collection of fresh blood clot on the right side outside the dura. |
|
K NS-105 |
|
Same case as K NS-104. The dura has been cut and the brain removed. Note extradural haemorrhage pushing dura of the convexity of the skull inwards. |
|
K NS-106 |
|
Same case as K NS-104 and 105. Coronal slice of brain. The right cerebral hemisphere has been indented by the extradural hematoma. The right lateral ventricle is slightly smaller than the left. Note small cortical contusion in cortex of left 3rd temporal gyrus (contrecoup ?). |
|
K NS-111, |
|
Two coronal views of the cerebrum and a view of three horizontal levels of the 112, 113 brainstem from session III, case 3. Note the swollen state of the cerebral hemispheres with small ventricles, prominent contusion of the corpus callosum, right temporal contusion and bilateral haemorrhagic occipital infarcts in posterior cerebral artery territory which are necessary to herniation. The hemorrhagic lesions in the brainstem are probably both direct injuries (contusions) and hemorrhages secondary to transtentorial herniation. |
|
K NS-114 |
|
Coronal section of brain with dura in place. A chronic subdural haematoma with the thick fibrous membranes is present. |
|
K NS-115 |
|
A myelin-stained section of the brain from case 5 of session III. Note the large ventricles, patchy myelin loss and more or less intact cortex. Bilateral thalamic atrophy is probably secondary to interruption of thalamo-cortical projection fibres. |
|
K NS-116 |
|
A diagrammatic representation of brain herniations resulting from an expanding intracranial lesion. |
|
Slide 121 |
|
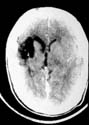
CT scan of brain, acute phase infarction |
|
Slide 122 |
|
coronal section of brain, acute infarction in the territory of the left middle cerebral artery. Please note that this pathology section has been reverted to correlate with the CT scan. |
|
Slide 123 |
|
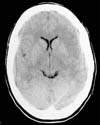
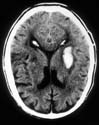
CT scan of brain, established infarct in the right middle cerebral artery territory. Note displacement of the mid-line. |
|
K NS 124 |
|
coronal section of brain. Established infarct with massive edema and displacement of the midline. Section has been reverted to correlate with the CT scan. |
|
K NS 125 |
|
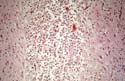
histological section of cerebral cortex. This section shows evidence of established ischemia. There is eosinophilic change, marked edema and prominence of endothelial cells. |
|
|
 |
CT scan of brain showing evidence of old infarction of the territory of the right middle cerebral artery. |
|
K NS 127 |
|
horizontal section through brain. Section has been reverted showing a cavitated infarct in the territory of the right middle cerebral artery to correlate with CT scan. |
|
K NS 128 |
|
microscopic sections through cavitated infarct. The cavity contains debris-laden macrophages. |
|
|

|
|
|
K NS 130 |

|
microscopic section through posterior cerebral artery showing an embolus |
|
|
|
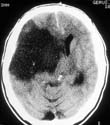
CT scan of brain showing a right basal ganglionic hemorrhage. |
|
K NS 132 |

|
horizontal section through brain showing a basal ganglionic hemorrhage. Section has been reverted to correlate with CT scan. |
|
K NS 133 |

|
microscopic section at the edge of the basal ganglionic hemorrhage. This slide is demonstrating a Charcot-bouchart aneurysm. |
|
|
|
CT scan of brain showing a lobar hemorrhage |
|
K NS 135 |
|