| -
The Heart
|
 |
|
Surface markings
|
What is the best landmark for marking the four points to draw the surface outline of the heart?
|

|
|
Incision on chest wall
|
Right pectoral muscles removed. Cut starting at manubrium, extending in the second intercostals space, laterally in mid axillary line and inferiorly along costal margin (taking care not to incise the underlying lung or diaphragm).
|

|
|
Thoracic cavity opened
|
Thoracic wall is removed by cutting the internal thoracic vessels and the mediastinal pleura as it reflects on to the ribs. The lungs are almost completely covering the heart.
|

|
|
Mediastinum, azygos vein
|
The right lung has been removed by cutting the structures at the hilum. Can you name them? The curved vein superior to the hilum is the azygos. It enters the SVC. The pericardium is intact. Inferiorly note the dome of the diaphragm.
|

|
|
Mediastinum, aortic arch
|
Removing the left lung by cutting the structures at the hilum exposes the aortic arch and the descending aorta. The pericardium is covered by the pleura. What innervates the fibrous pericardium?
|

|
|
Sternocostal surface of heart
|
Part of the pericardium is incised and removed, revealing the sternocostal surface of the heart. So called as it underlies the sternum and the ribs. Name the structures forming the right, inferior and left border of the heart. To the right of the apex, a branch of the left coronary artery is faintly visible. What better name than left anterior descending for it!
|

|
|
Transverse sinus
|
The forceps is in the transverse sinus of pericardium. Anterior to it are the aorta and the pulmonary trunk. It is due to folding of the embryonic heart tube. It is often used to tie a ligature during bypass surgery.
|

|
|
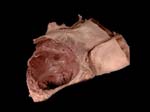
Oblique sinus
|
The heart has been removed by cutting the vessels (SVC, aorta, pulmonary trunk, pulmonary veins and IVC). The space bound by the IVC and the right pulmonary veins (in the lower part of the image) and the left pulmonary veins, is the oblique sinus of pericardium. Before the heart was removed, my fingers could trace the cul de sac! The left atrium, occupying most of this space forms the base of the heart.
|

|
|
Posterior mediastinal structures
|
(The image is rotated 90 degrees as compared to the previous one so that the head is at the top of the screen.) Removal of pericardium and further dissection exposes the trachea, esophagus and azygos. Part of the pericardium is still attached to the diaphragm. Can you identify the nerve anterior to the left main bronchus? How about the one around the aortic arch?
|

|
|
Vagi and recurrent laryngeal nerves
|
Lying on the black cloth from right to left are the right vagus, right recurrent laryngeal, trachea, left recurrent laryngeal and left vagus. The left recurrent goes around the ligamentum arteriosum (aortic arch). What does the right hook around? The vagus is situated posterior to the hilum.
By the way the phrenic which lies anterior to the hilum, innervates the pericardium (not the visceral, and what else?).
|

|
|
Sternocostal surface
|
The heart removed from the cavity. The parietal pericardium is also removed. (The visceral is adherent to the heart and forms the epicardium.) Note the right atrium, right auricle, right ventricle and the left ventricle. The vessels seen are the right pulmonary artery, SVC, aorta with its branches and pulmonary trunk leading to the left pulmonary artery. There are two bands of fat covering the atrio-ventricular and anterior inter-ventricular grooves.
|

|
|
Base and diaphragmatic surface
|
The big black hole is the IVC. Just above are four pulmonary veins entering the left atrium. The curvy structure between the atria and left ventricle is the coronary sinus. Also note how the pulmonary trunk divides into two in the aortic arch.
|

|
|
Looking from above
|
From above down note the aorta, pulmonary arteries and openings of the pulmonary veins. What is the space between the pulmonary arteries and veins? Starts with a T!
|

|
|
Auricles
|
The only things clearly visible are the branches from the aortic arch and the auricles. The auricles resemble a dog’s ear and are derived from primitive atria. There is a lot more fat as compared to the previous heart.
|

|
|
Coronary sinus
|
Can you visualize its location? What does it do? Note the IVC opening and the vessels in the posterior inter ventricular groove.
|

|
|
Pulmonary and aortic semilunar valves
|
Opening of the pulmonary trunk and aorta is guarded by a valve with three semilunar cusps. As ventricles relax blood fills these cusps and closes the opening. This photo shows the SVC (on the right of the screen), the aorta in the middle and the pulmonary trunk on the left.
|

|
|
Right coronary artery
|
Removing the fat and reflecting the right auricle exposes the right coronary and some of its branches. It takes origin from the right aortic sinus. Aortic sinus is a dilatation of the aortic wall opposite the cusp.
|

|
|
Left coronary artery
|
Left auricle is retracted to show the left coronary. It arises from the left coronary sinus and divides soon after into two almost equal branches. One descending between the two ventricles anteriorly is the left anterior descending. Curving around in the coronary /atrioventricular sulcus is the circumflex branch. These coronary arteries are the sole arterial supply to the heart muscle. What part does each supply?
|

|
|
Coronary sinus and right posterior descending
|
Can you identify the IVC, the coronay sinus, the right posterior descending artery accompanied by the middle cardiac vein and the marginal branch of the right coronary? (start at the IVC, go to the left of the screen and move to the right)
|

|
|
Right and left coronary
|
This is a cast of the right and the left coronary arteries and their branches. Note how the right supplies mainly the right side and the left mainly the left side but also some right. Do the coronary arteries anastomose?
|


|
|
Fossa ovalis and musculi pectinate
|
Looking into the right atrium you see the fossa ovalis, a saucer shaped depression on the interatrial septum. What is it a remnant of? If there was a hole in its place, what effect would it have on blood circulation? The parallel muscular ridges seen on the flap resemble a comb and are hence called musculi pectinate. (Remains of the primitive right atrium.)
|

|
|
Coronary sinus opening
|
The little opening (on the lower right part of the screen) admits the tip of owners little finger and is located a little to the left side of the IVC. It is guarded by the valve of the IVC.
|

|
|
AV valves
|
Parts of the atria and the great vessels have been cut. The AV valves guard the openings between the atria and the ventricles. The one on the right side has three cusps and is hence called the tricuspid valve. The one on the left has two cusps and resembles a bishop’s miter, so it is called the mitral/bicuspid valve. Note that the cusps are smooth (no chordae are attached to the atrial surface).
|

|
|
Semilunar valves
|
If the aortic or the pulmonary valve does not close completely when the ventricle relaxes, what would be the result on the blood flow? In this specimen the tricuspid as well as the pulmonary semilunar valves are open.
|

|
|
Aortic regurgitation
|
Failure of the aortic valve to close completely during ventricular diastole results in aortic regurgitation (blood leaking through the aortic valve). This back flow produces a characteristic murmur. The big red mass seen in the middle is due to the injected material leaking through the aortic valve.
|


|
|
Right ventricle – internal features
|
Note the inelastic chordae tendineae extending from the finger like projections called the papillary muscles. The smooth area leading to the pulmonary opening is the infundibulum. It neither contracts nor relaxes.
|

|
|
Left ventricle – internal features
|
The left ventricular wall is a lot thicker than the right. There are two papillary muscles. The chordae from each muscle go to both the cusps. When the ventricle contracts it pulls the cusps together, thus closing the opening. Ineffective closure of the mitral valve results in mitral regurgitation (blood gushing back into the atrium during ventricular systole).
|

|
|
VSD and coronary bypass
|
A square window cut in the interventricular septum. Sometimes there is a congenital defect called VSD (hole in the IV septum). Loop on the upper right side is a vessel attached to bypass the blocked part of a coronary artery.
|

|
|
Coronary bypass and artificial mitral valve
|
Note the stitches where one end of the graft vessel was attached to the aorta. The mitral valve has been replaced by a metal ring.
|

|
|
Normal or abnormal?
|
What is the most significant abnormality seen in this heart? Answer - A bypass vessel crossing the pulmonary trunk to connect to the LAD.
|

|
|
What surfaces?
|
Which areas can you identify? Answer – Base and diaphragmatic surface. Why can this not be the sternocostal surface?
|

|
|
Moderator band
|
A bundle of muscle fibers connects the septum to the base of the anterior papillary muscle and is hence called septomarginal band. When present (60 % of hearts) it transmits the right branch of the bundle of his. So it is also known as the moderator band.
|

|
|
SA node
|
Where is the SA node – the pacemaker located? It is hard to see in human hearts. It is located a little to the left of the sulcus terminalis (faint line seen on the surface of the right atrium where the crista terminalis is on the inside) near the SVC opening. (Crista is the dividing line between the part of the atrium that develops from the primitive atrium and the one that forms from sinus venarium.)
|

|
|
AV node
|
The AV node is located in the interatrial septum (close to the coronary sinus opening). The impulse is transmitted from the SA node to the AV node by the heart muscle itself.
|

|
|
Bundle of His
|
It is the sole muscular connection between the atria and the ventricles. It is a specialized bundle of fibers that transmit the impulse from the AV node to the base of the papillary muscles and the ventricle walls. It travels in the IV septum and soon divides into two branches. The left branch continues in the septum to the left ventricle.
|

DSCN0178 (need to take)
|
|
Right bundle branch
|
The right branch passes in the moderator band (when present) to the right ventricle.
|

|
|
What slows the heart?
|
Parasympathetic fibers in vagi, (synapse in the ganglia on the atrial wall and cardiac plexuses) cause a decrease in the heart rate.
|

|
|
What causes the heart to beat fast?
|
Sympathetic fibers increase the heart rate. Cell bodies of the preganglionic fibers are in the T1-T4 segments of the spinal cord. Fibers synapse in the cervical chain ganglia. Postganglionic fibers from here go via the cardiac plexuses to innervate the heart.
|

|
|
Which chamber?
|
The right atrium. If the foramen ovale did not close, what is the clinical condition called? Name one physical finding that the patient may present with.
|
|
|
Cardiac veins
|
These drain the heart muscle itself. Most cardiac veins (60 %) drain into the coronary sinus.
|

|
|
Anterior cardiac veins
|
A few cardiac veins on the anterior surface of the heart drain directly into the right atrium
|

|
|
LAD
|
Does this artery anastomose? Where and with which artery?
|

|
|
Name arteries that anastomose in the AV groove
|
The circumflex branch of the left coronary anastomoses with the right coronary after the posterior interventricular has been given off.
|

|
| -
The Heart
|
 |
|